
Why This Matters:
- Time-to-therapy is critical for Gram-negative bloodstream infections: Rapid phenotypic Antimicrobial Susceptibility Testing (AST) can materially influence outcomes.
- Conventional AST: Traditional workflows require subculture and overnight incubation, often delaying susceptibility results by 24–48 hours.
- Direct-from-blood-culture AST: bypass full subculture, providing MIC-based susceptibility results within the same shift.
- Antimicrobial stewardship impact: Earlier susceptibility data supports de-escalation from broad-spectrum empiric therapy, reducing toxicity, resistance selection, and costs.
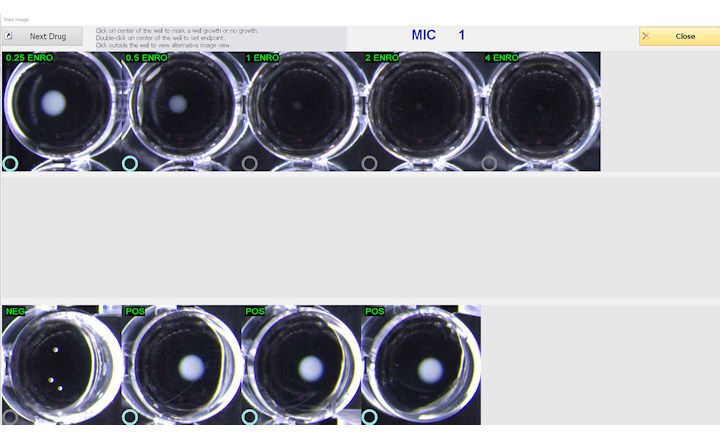
Key Findings: Simmons-Williams et al. evaluated rapid Antimicrobial Susceptibility Testing (AST) performance of VITEK REVEAL and Accelerate Pheno using 128 monomicrobial Gram-negative blood cultures across 1,410 organism–antimicrobial combinations.¹ The study focused on analytical performance; cost, hands-on time, and laboratory integration were not formally assessed but remain critical adoption variables.
- Time to result (TTR): VITEK REVEAL = 7.9 h vs Accelerate Pheno = 7.1 h. Although Accelerate produced a slightly shorter final TTR, VITEK REVEAL delivered actionable MICs earlier on a per-drug basis.
- Agreement metrics:
- Categorical agreement: 94.3%
- Essential agreement: 96.0%
- Very major discrepancy: 7.5%
- Major discrepancy: 0.5%
- Minor discrepancy: 4.1%
- Discrepancy patterns: Lower agreement was observed for certain β-lactam/organism combinations (e.g., ampicillin-sulbactam, select Pseudomonas spp. isolates). Some minor discrepancies reflected undercalling of resistance (intermediate vs. resistant), which may have stewardship implications.
Bigger Picture: Rapid phenotypic AST platforms are narrowing the time gap between blood culture positivity and targeted therapy. This study demonstrates that both VITEK REVEAL and Accelerate Pheno achieve high agreement and sub-8-hour reporting in Gram-negative blood stream infections. In institutions with active antimicrobial stewardship programs, even a 1–2 hour earlier actionable result can alter escalation/de-escalation decisions during the same clinical shift. Future evaluations should incorporate clinical outcome measures (time to optimal therapy, length of stay, mortality), cost-effectiveness analyses, and performance against reference broth microdilution standards to fully define comparative value.
(Image Credit: iStock/ Md Saiful Islam Khan)