Nearly half of child deaths under five are caused by neonatal sepsis and despite enhancements in knowledge of other fatal childhood illnesses, neonatal sepsis is still overlooked1.
Neonatal sepsis is characterised by infection of the bloodstream; there are two different types including early-onset sepsis (EOS), which occurs before 72 hours of life and late-onset sepsis (LOS), which occurs after 72 hours of life2. EOS is typically caused by transmission of pathogens such as group B Streptococcus, Escherichia coli and Listeria monocytogenes from the female genitourinary system to the newborn or foetus, whereas LOS is usually caused by transmission of pathogens such as coagulase-negative Staphylococci post-birth or during birth2.
Since the 1990s, EOS has declined but LOS rates have not generally changed, encouraging scientists to improve their understanding of the infection and establish a possible cause2.
Over the decades of research into neonatal sepsis, scientists have found that the gut microbiome plays a vital role in neonatal health3. Gut pathogen colonisation can be a precursor to many infections in neonates, so understanding gut dysbiosis and sepsis is paramount for preventative and therapeutic strategies3.
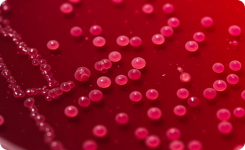
Iqbal et al. investigated the difference in the gut microbiota of babies who developed sepsis compared to those who did not3. Faecal samples were collected on day 4 of life from 182 preterm neonates (91 who had sepsis and 91 without sepsis) and incubated at 37oC for 24 to 48 hours. For efficient growth of any anaerobes, the samples were inoculated on 5% sheep blood agar and neomycin blood agar with a metronidazole disc and incubated in a Whitley A35 Workstation3.
For infants without sepsis, faecal samples were also taken on day 14 but the second sample for those with sepsis was taken when blood culture bottles showed growth of pathogenic bacteria3. Evidence shows that there is a difference in gut microbiome depending on whether the babies have sepsis or not as on day 14, there was a significant difference in E. coli with 64.7% cultured from those diagnosed with sepsis, compared to 50% in those without sepsis3. Similarly, there were much higher rates in those with sepsis for other bacteria including Bifidobacterium spp. and Klebsiella pneumoniae, compared to those without sepsis [3].
Among these findings, they also discovered microbial differences depending on the mode of delivery; for vaginal births, there was a higher prevalence of beneficial gut flora bacteria such as Bifidobacterium spp. and Enterococcus faecalis compared to caesarean section births3.
Written by DWS Microbiologist, Kirsty McTear
Click here to see the Whitley Anaerobic Workstation range
References
1. Strunk T, J Molloy E, Mishra A, Bhutta ZA. Neonatal bacterial sepsis. The Lancet. 2024 May 26;404(10449):277–93.
2. Singh M, Alsaleem M, Gray CP. Neonatal Sepsis. [Updated 2022 Sep 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from here.
3. Iqbal F, Shenoy PA, Siva N, Vandana KE, Purkayastha J, S. Lewis LE. From dysbiosis to disease: Tracing gut microbiota’s role in neonatal sepsis. Clinical Epidemiology and Global Health. 2024 Oct 8;30:101809.